Why Your Inflammation Marker Matters More Than Your Cholesterol

Why Your Inflammation Marker Matters More Than Your Cholesterol
I've been getting blood work done for years. Every time, same thing — cholesterol, blood sugar, liver, kidney, blood cells. My doctor looks at the numbers, flags anything high, and we move on.
Not once did anyone order an inflammation marker.
I didn't even know there was a blood test that could measure how much inflammation is in your body. Nobody told me. It never came up. And honestly, that bothers me — because it turns out this might be the most important number on a blood panel.
The test is called hs-CRP — high-sensitivity C-reactive protein. And when I finally got it tested, the result came back: <0.2 mg/L.
That's not just low. That's undetectable. The lab literally couldn't measure it — the result is reported as "less than 0.2" because my level is below the test's detection threshold. The machine looked for inflammation in my blood and found nothing to register.
Here's the scale for cardiovascular risk:
- <1.0 mg/L — Low risk
- 1.0–3.0 mg/L — Moderate risk
- >3.0 mg/L — High risk
I'm not in the low-risk category. I'm below the floor of the low-risk category. My body has so little systemic inflammation that the most sensitive version of the test can't quantify it.
And I had no idea this marker even existed until I ordered my own labs.
Meanwhile, My Cholesterol Looks "Bad"
On the same blood panel:
- LDL cholesterol: 184 mg/dL — flagged high (reference: <100)
- Total cholesterol: 259 mg/dL — flagged high (reference: <200)
If my doctor had only ordered the standard panel — which is exactly what happened on my last visit — the conversation would have been: "Your cholesterol is high, let's talk about statins."
But with the inflammation marker, the picture changes completely.
How Cholesterol Became the Default — and Why It Shouldn't Be
Cholesterol became the go-to marker for heart health because it was easy and early — not because it was the best.
The cholesterol hypothesis took off in the 1960s and '70s. It was measurable, it correlated with heart disease in population studies, and — crucially — there were drugs that could lower it. Statins arrived in the late 1980s and became one of the most prescribed drug classes in history. The entire cardiovascular prevention framework was built around one question: what's your cholesterol?
But here's the thing — cholesterol is a building material. Your body uses it constantly for hormones, cell membranes, and brain function. It's circulating in your blood all the time. That's normal. About half of people who have heart attacks have normal cholesterol levels. That alone should tell you the model is incomplete.
Cholesterol doesn't clog your arteries on its own.
The problem starts when the walls of your arteries get damaged. And the primary thing that damages them is inflammation.
When arterial walls are inflamed, LDL particles penetrate into the wall and get trapped. Your immune system responds by sending white blood cells, which consume the LDL, swell up, and die — forming the fatty plaques that narrow arteries. Without that initial inflammatory damage, cholesterol largely passes through without causing harm.
This isn't fringe science. This is decades of research:
-
A landmark 2002 study followed 27,939 healthy women for eight years and found that C-reactive protein is a stronger predictor of cardiovascular events than LDL cholesterol. The two markers identified different high-risk groups — measuring both was better than measuring either alone. (Ridker et al., 2002)
-
The JUPITER trial (17,802 participants) showed that people with normal cholesterol but elevated hs-CRP still benefited from treatment — because the inflammation itself was the risk. The trial was stopped early because the results were so clear. (Ridker et al., 2008)
-
A 2023 meta-analysis of statin-treated patients found that hs-CRP was a more potent predictor of future cardiovascular risk than LDL cholesterol — even in patients already on aggressive cholesterol-lowering therapy. Cardiovascular death and all-cause mortality were more than twice as high among those with the highest CRP levels compared to those with the highest cholesterol levels. (Ridker et al., 2023)
-
A 30-year follow-up study tracked 27,939 women and found hs-CRP predicted cardiovascular events with a hazard ratio of 1.70 — compared to 1.36 for LDL cholesterol and 1.33 for lipoprotein(a). (Ridker et al., 2024)
The research is consistent: inflammation predicts heart disease at least as well as cholesterol — and in many studies, better.
So Why Didn't My Doctor Order This?
This is the part that frustrates me. The American College of Cardiology released a scientific statement in 2025 that now recommends universal screening of hs-CRP in both primary and secondary prevention. Their exact words: "Because clinicians will not treat what they do not measure, universal screening of hsCRP in both primary and secondary CVD prevention represents a major clinical opportunity and is therefore recommended."
But most doctors still don't order it. Here's why:
-
It's not on the default panel. Standard blood work includes lipids, metabolic markers, and CBC. hs-CRP requires a separate order. If the doctor doesn't actively add it, you don't get it.
-
It's nonspecific. A high hs-CRP tells you something is inflamed but not what or where. Doctors trained to find specific diagnoses sometimes dismiss markers that don't point to a single cause.
-
Old guidelines didn't recommend it broadly. Until recently, hs-CRP was only suggested for patients at "intermediate" cardiovascular risk. The 2025 ACC statement changes this, but guideline changes take years to reach your local doctor's office.
-
The standard cholesterol conversation is easier. High cholesterol → statin prescription. It's a well-worn path with a clear drug at the end of it. Adding inflammation to the conversation makes things more nuanced — and the answer might be lifestyle changes instead of a prescription. That's a harder conversation in a 15-minute appointment, and there's no pharmaceutical company funding awareness campaigns for "train your nervous system."
My May 2025 labs — ordered by my doctor at Cedars-Sinai — included a full lipid panel, CBC, metabolic panel, thyroid, liver, kidney function. Standard stuff. No hs-CRP. No inflammation marker of any kind.
When I ordered my own comprehensive panel in March 2026 through Quest Diagnostics, I specifically included hs-CRP. That's the only reason I have this number.
What My Blood Work Actually Shows
Here's the full picture with inflammation included:
| Marker | My Value | Reference | What It Means |
|---|---|---|---|
| hs-CRP | <0.2 mg/L | <1.0 low risk | Undetectable — below test threshold |
| LDL Cholesterol | 184 mg/dL | <100 | Flagged high |
| Total Cholesterol | 259 mg/dL | <200 | Flagged high |
| Triglycerides | 87 mg/dL | <150 | Good |
| HDL Cholesterol | 55 mg/dL | >40 | Good |
| Fasting Insulin | 8.0 uIU/mL | <18.4 | Optimal |
| Fasting Glucose | 95 mg/dL | 65-99 | Normal |
Elevated cholesterol with high inflammation is a well-documented cardiovascular risk combination — the fire and the fuel together. But elevated cholesterol without inflammation? That's a fundamentally different risk profile. The fuel is there, but there's no fire.
This doesn't mean high LDL is harmless — I'm still monitoring it and pursuing further testing (ApoB, coronary calcium score). But the conversation is completely different when you know your inflammation is undetectable versus when you're guessing.
How Unusual Is This? — Population Data
To understand what <0.2 mg/L actually means, you need to see what normal looks like. The best data comes from NHANES (National Health and Nutrition Examination Survey) — the CDC's massive ongoing study of American health, analyzing 21,004 people (Rifai et al., 2005):
| Population | Median hs-CRP |
|---|---|
| Me (age 44) | <0.2 mg/L |
| U.S. adults age 20–29 | 1.4 mg/L |
| U.S. adult men (all ages) | 1.6 mg/L |
| U.S. adults overall | 2.1 mg/L |
| U.S. adult women (all ages) | 2.7 mg/L |
| U.S. adults age 80+ | 2.7 mg/L |
| Chinese adults age 40–59 (longevity areas) | 0.99 mg/L |
The median American adult walks around at 2.1 mg/L. I'm at <0.2. That's more than 10x lower than the typical American.
52% of American adults have hs-CRP at or above 2.0 mg/L — the threshold the American Heart Association considers elevated cardiovascular risk. More than half the country is walking around with active systemic inflammation and most of them have no idea, because nobody ordered the test.
The cardiovascular risk tiers put this in perspective:
- <1.0 mg/L — Low risk
- 1.0–3.0 mg/L — Moderate risk (this is where the average American sits)
- >3.0 mg/L — High risk
The average American is in the moderate risk category by default. Just by existing in modern life, eating a standard diet, sleeping a standard amount, and carrying standard stress levels.
Here's what makes this even more striking: a study of adults aged 40–59 living in designated longevity areas of China — the closest thing to Blue Zone population data with hs-CRP numbers — found a median of 0.99 mg/L (Huang et al., 2018). These are people living in communities specifically identified for exceptional lifespan. Even they are roughly 5x higher than my result.
I'm not matching longevity populations. I'm below them. In modern Los Angeles, at age 44, eating a decent but not perfect diet.
And I didn't get here through dietary perfection or genetic luck. I got here by training my nervous system. That distinction matters — and I'll explain why below.
What Drives Inflammation Up
Chronic low-grade inflammation — the kind hs-CRP catches — builds silently from things most people do every day:
- Ultra-processed food: Refined sugar, seed oils, and artificial additives trigger inflammatory pathways
- Poor sleep: Sleep deprivation elevates inflammatory cytokines (IL-6, TNF-alpha) within days
- Chronic stress: Sustained cortisol output eventually becomes pro-inflammatory
- Sedentary behavior: Lack of movement reduces anti-inflammatory myokine production
- Visceral fat: Belly fat is metabolically active and secretes inflammatory compounds continuously
- Gut dysfunction: A compromised gut barrier lets bacterial endotoxins leak into circulation
Most of this is invisible. You feel fine. Your doctor checks your cholesterol, maybe your blood sugar. But inflammation can be building for years before it shows up as disease.
What I Think Drove Mine So Low — I'm Training My Heart Every Day
Here's what I think people miss: cardiovascular health isn't just about what's in your blood. It's about whether you're training the system.
Think about what your heart actually does. It pumps blood. Every beat pushes blood through your entire circulatory system — through your arteries, into your capillaries, back through your veins, through your lungs for oxygen, and back out again. The harder you work, the faster it pumps. The more blood moves through, the more your vascular system gets used, maintained, and kept elastic.
Your cardiovascular system is adaptive. If you never stress it, it weakens. If you stress it strategically, it gets stronger. And the inflammation marker reflects how well that system is functioning.
I'm running blood through my heart at high rates multiple times a day — through completely different mechanisms. And the order matters. Here's the actual sequence:
Breathwork — this is where the session starts. Wim Hof-style breathing with a unique "gasp" inhale technique — a rapid sucking motion, like the breath you'd take before saying "oh no she didn't." Full exhale, repeat 30-40 times per round, 2-3 rounds. This directly drives heart rate up and down. Inhale: sympathetic activation, heart rate rises. Exhale: parasympathetic activation, heart rate drops. My heart rate swings from 72 to 101 BPM just from breathing — no movement at all. And after power breathing sessions, my overnight HRV has jumped as much as 250% (30 ms to 105 ms). That's the parasympathetic rebound — the nervous system recovering stronger than before, like a muscle after a workout. The breathwork also creates a hypoxic state that primes everything that comes next.
Breathwork and hypoxic training: heart rate oscillation driven purely by breath — no movement required.
Cold exposure — immediately after breathwork, I step into an ice shower at 35°F for 2-5 minutes. My heart rate spikes, my blood vessels constrict, and my sympathetic nervous system fires hard. Blood is being pumped fast. Then I regulate — my body practices going from stress to recovery. That oscillation trains vagal tone, which is the strength of your parasympathetic nervous system. Higher vagal tone is directly associated with lower inflammation. I'm not just "taking a cold shower." I'm doing cardiovascular interval training without running a single step.
Cold exposure session: heart rate spike and recovery. Same cardiovascular training effect as interval running — different mechanism.
Short intense movement — breath-hold sets of burpees, Hindu squats, or Wim Hof push-ups, 6 sets to form breakdown. This is hypoxic training — exercising while the body is still in a low-oxygen state from the breathwork and cold. The combination creates extreme EPOC (excess post-exercise oxygen consumption) that keeps metabolism elevated for 24-48 hours.
Walking at 140-150 BPM — here's the one that surprises people. Right after the hypoxic movement, I walk on an incline treadmill for 35 minutes. Just walking. But because my nervous system is still in a heightened state from the cumulative effect of breathwork, cold, and hypoxic movement, my heart rate sustains 140-150 BPM for the entire 35 minutes. It feels like a normal easy walk — my perceived exertion is low — but my heart is pumping like I'm running. That's 35 minutes of sustained high-output blood flow through my entire cardiovascular system, every session. Without the prior sequence, the same walk would be 80-100 BPM. With it, I'm getting a cardiovascular training effect from walking.
Just walking — but the cumulative priming from breathwork, cold, and hypoxic movement keeps my heart rate at 140-150 BPM for 35 minutes. Cardiovascular training effect from an easy walk.
Heat exposure — after the walk, sauna pushes heart rate up through a completely different mechanism than exercise. Your body vasodilates to dump heat, blood rushes to the skin surface, and your heart has to pump harder to maintain blood pressure. More blood flowing, different pathway, same training effect on the cardiovascular system.
Sauna: cardiovascular demand through a completely different mechanism — vasodilation rather than muscular effort.
The spontaneous override — here's something wild I've documented: during one of these incline walks, my heart rate dropped from 144 to 106 BPM in about 75 seconds. I didn't slow down. I didn't change my breathing. Same pace, same incline. My autonomic nervous system just decided it didn't need to run that hot anymore and shifted the set point down by nearly 40 BPM. That's not something an untrained nervous system does. That's a system that has enough control to modulate its own output in real time.
Every one of these pushes blood through my heart at elevated rates — and the sequence builds on itself. Breathwork primes the nervous system. Cold sharpens it. Hypoxic movement creates the metabolic demand. Walking sustains the elevated output. Heat amplifies the recovery. Five different stimuli, five different mechanisms, all training the same pump. My heart isn't sitting idle waiting for a weekend jog. It's working, recovering, working, recovering — all day.
Why This Actually Trains the Heart
Here's what's happening at the tissue level when you repeatedly push blood through your cardiovascular system at elevated rates:
Shear stress keeps your arteries healthy. When blood flows fast, it creates friction against the inner walls of your arteries — the endothelium. That friction is called shear stress, and it's not damage. It's a signal. Your endothelial cells respond to shear stress by producing nitric oxide (NO), which does three critical things: it relaxes and dilates your blood vessels, it prevents white blood cells from sticking to arterial walls (the first step in plaque formation), and it inhibits smooth muscle proliferation that thickens artery walls. Regular high-flow episodes keep this signaling pathway active. Without them, it goes quiet — and that's when arteries start stiffening and inflammation creeps in.
Your heart is a muscle — it adapts to demand. When you sustain elevated heart rates (like 140-150 BPM for 35 minutes), your heart has to move more blood per minute. Over time, the left ventricle adapts by increasing its stroke volume — pushing more blood per beat. This is why trained hearts are more efficient at rest: they can deliver the same cardiac output with fewer beats. Lower resting heart rate, higher HRV, better recovery — all downstream effects of a heart that's been given regular work to do.
You're training the entire vascular tree, not just the heart. Arteries, arterioles, capillaries, venules, veins — the whole network responds to increased blood flow. Capillary density increases in tissues that are regularly perfused at high rates. Arterial walls maintain their elasticity instead of stiffening with age. The smooth muscle in your vessel walls stays responsive. This is why cardiovascular training reduces blood pressure over time — your vessels literally become better pipes.
The anti-inflammatory effect is direct. Contracting muscles during exercise release myokines — signaling molecules that actively suppress inflammation. IL-6 released during exercise (which is different from the IL-6 released during chronic inflammation) triggers a cascade that increases anti-inflammatory cytokines (IL-10, IL-1ra) and decreases pro-inflammatory ones (TNF-alpha). Every session is an anti-inflammatory treatment. But here's the key — I'm not just getting this from one bout of exercise. I'm getting it from cold, from breathwork, from walking, from heat. Multiple anti-inflammatory signals, multiple times a day.
Recovery is where the adaptation happens. The oscillation matters as much as the stress. Going from high sympathetic activation (cold plunge, breathwork) to parasympathetic recovery trains your vagus nerve — the main brake pedal of your nervous system. Stronger vagal tone means faster recovery, lower baseline inflammation, and a heart that can shift gears efficiently. This is what HRV measures: how well your heart can vary its rhythm in response to changing demands.
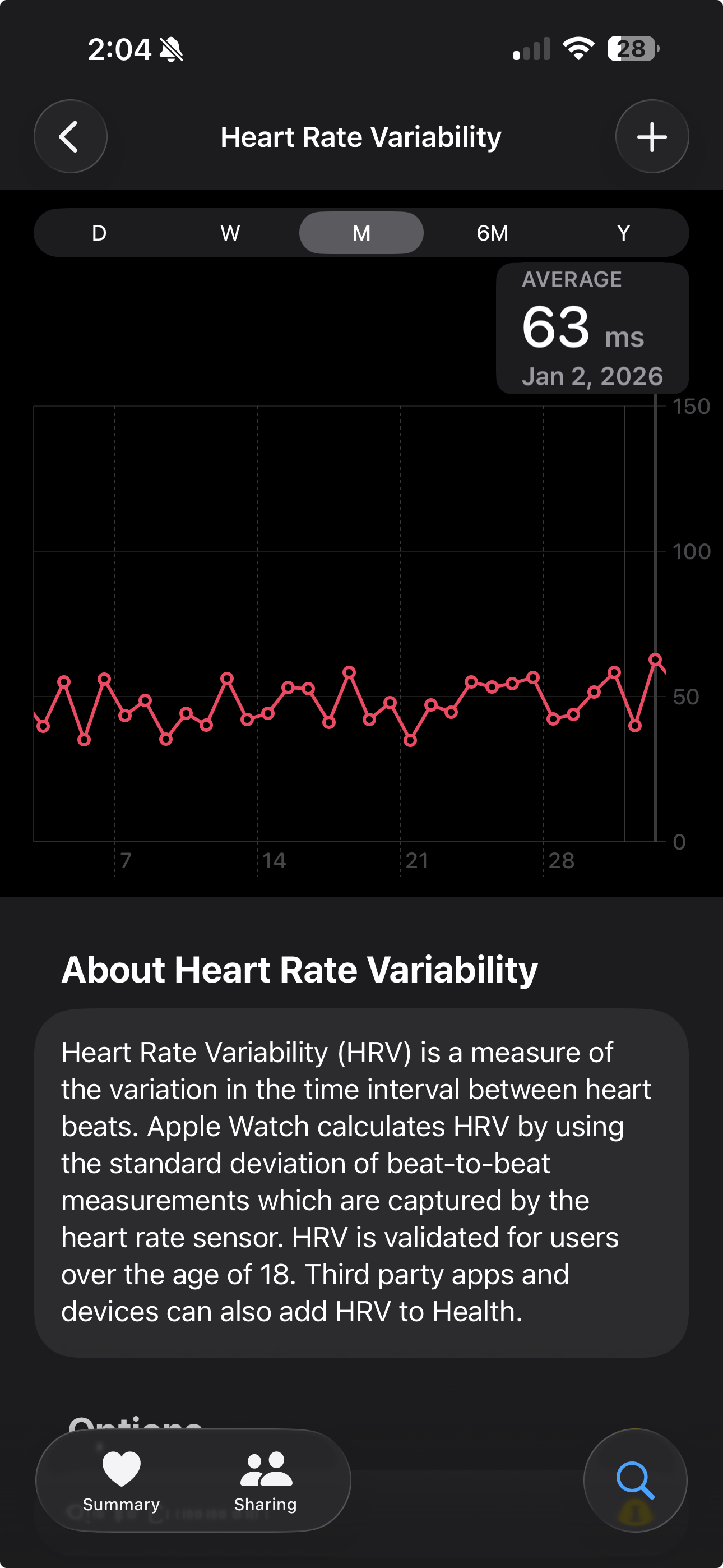
My HRV jumps of 250% after breathwork sessions aren't random — they're the parasympathetic rebound getting stronger with training.
The net result: my cardiovascular system is being maintained the way it was designed to be — through regular, varied demand. The undetectable hs-CRP isn't despite all this stress on the system. It's because of it. A cardiovascular system under regular adaptive stress doesn't accumulate chronic inflammation. It clears it.
The Other Factors Completing the Picture
Time-restricted eating (16-18 hour daily fasts) — fasting gives the gut regular rest periods, reduces inflammatory burden, and improves insulin sensitivity. My fasting insulin is 8.0 and my triglycerides are 87 — both markers of a metabolic system that's running clean.
Sleep quality — my sleep efficiency runs 96-100% with near-zero wake time during the night. And here's the thing: the hs-CRP result independently proves the sleep data is real.
People can question wearable accuracy. "Your watch overestimates sleep quality." "Nobody actually sleeps at 96-100% efficiency." Fine — but the blood doesn't lie. The research on sleep and inflammation is direct (Irwin et al., 2006):
- Sleep deprivation — even one bad night — elevates inflammatory cytokines (IL-6, TNF-alpha) and raises CRP
- Chronic sleep fragmentation keeps those markers elevated indefinitely
- The glymphatic system — the brain's waste removal process — runs primarily during deep, unbroken sleep. If sleep is fragmented, inflammatory metabolites accumulate instead of being cleared
- Overnight cortisol is supposed to drop to its lowest point during consolidated sleep. Fragmented sleep prevents that full suppression, and elevated overnight cortisol is directly pro-inflammatory
If my sleep were secretly bad, my hs-CRP would show it. There is no version of reality where someone sleeps poorly and maintains undetectable systemic inflammation. Work it backwards:
| If this were true... | hs-CRP would be... | My hs-CRP is... | Therefore... |
|---|---|---|---|
| Sleep is fragmented | Elevated (1.0+) | <0.2 | Sleep is not fragmented |
| Sleep efficiency is overstated by watch | Elevated | <0.2 | Watch data is accurate |
| Deep sleep is insufficient | Elevated | <0.2 | Deep sleep is sufficient |
| Overnight recovery is incomplete | Elevated | <0.2 | Recovery is completing fully |
A clinical blood test just confirmed what a consumer wearable has been reporting for months. Two completely different measurement methods — clinical chemistry and wrist-based sensors — arriving at the same conclusion: this sleep is genuinely, measurably restorative.
And I didn't try to sleep this way. I didn't follow sleep hygiene protocols, set a strict bedtime, optimize my bedroom temperature, or buy a special mattress. My nervous system just started sleeping correctly on its own after I trained it.
Visceral fat loss — before the protocol, I carried visceral fat. After it, most or all of it is gone. I didn't diet to lose it. I didn't count calories. The nervous system training changed my body composition — and the hs-CRP confirms it.
Here's why this matters: visceral fat isn't passive storage. It's classified as an endocrine organ because it actively secretes inflammatory compounds around the clock — TNF-alpha, IL-6, resistin, excess leptin, and PAI-1. Roughly 30% of all circulating IL-6 in the body comes from visceral fat alone, and IL-6 is the cytokine that travels to your liver and directly stimulates CRP production.
If I still had significant visceral fat, my hs-CRP could not be <0.2. The fat would be producing inflammatory cytokines whether I wanted it to or not. And every other metabolic marker corroborates this:
| Marker | My Value | What It Confirms |
|---|---|---|
| hs-CRP | <0.2 mg/L | No inflammatory source present — visceral fat gone |
| Fasting Insulin | 8.0 uIU/mL | Insulin sensitive — not in fat-storage mode |
| Triglycerides | 87 mg/dL | Clean metabolic processing — no excess lipid circulation |
| Fasting Glucose | 95 mg/dL | Normal — no insulin resistance |
If visceral fat were still there, you'd expect at least one of these to be off. All four are clean. That's not one marker suggesting the fat is gone. That's four independent markers confirming it.
The nervous system connection is direct: visceral fat accumulation is driven by cortisol and sympathetic nervous system dominance. Chronic stress → sustained cortisol → cortisol specifically directs fat storage to the visceral compartment. Sympathetic dominance → insulin resistance → the body stays locked in fat-storage mode. When I trained my nervous system out of sympathetic dominance, cortisol regulation improved, insulin sensitivity improved, and my body stopped getting the signal to store visceral fat — and started mobilizing it instead.
None of these are medications. They're demands on the system — the kind of demands that make it stronger.
That's what hs-CRP <0.2 reflects. Not the absence of stress — the mastery of it.
What This Number Actually Represents
Let me step back from the science for a moment.
A year ago I was dealing with job loss, depression, and a body I didn't recognize. I had belly fat I couldn't explain, energy that crashed by noon, and sleep that left me more tired than when I'd gone to bed. I wasn't eating terribly. I wasn't a couch potato. But something was off, and the standard blood work never flagged it.
The hs-CRP number doesn't just tell me my arteries are healthy. It tells me that the protocol I've been running — the cold exposure, the breathwork, the hypoxic walks, the fasting, the sleep — is actually doing something real at the cellular level. It's not in my head. It's not just better energy and better mood. The blood doesn't lie.
What surprised me most isn't the number itself. It's how I got there. I didn't "optimize" my inflammation. I didn't take a supplement stack and wait. I trained my nervous system — and my cardiovascular system came along as a passenger. The sleep corrected itself. The visceral fat left. The inflammation disappeared. Not because I targeted any of them directly, but because I addressed the root.
Your nervous system is the control system for all of it.
Ask for This Test
If you're getting blood work done, ask your doctor to add hs-CRP. If they won't, you can order it yourself through direct-to-consumer labs like Quest or Ulta Lab Tests for about $20-40.
If you've been told your cholesterol is high, this number adds the context that cholesterol alone can't give you:
- High cholesterol + high hs-CRP = the fire and the fuel are both present. Act now.
- High cholesterol + low hs-CRP = the fuel is there but there's no fire. Different conversation.
Either way, you deserve to know. I just wish someone had told me about it sooner.
And if you want to know what moves the number — not just supplements and diet, but actually training the system that controls it — that's what the CryoForge protocol is documenting. Real data, one person's experiment, no perfection required.
There's another piece of this puzzle I'm pursuing: coronary artery calcium. Inflammation drives calcium into your arterial walls — and there's a natural protocol for stopping it and routing calcium where it actually belongs. I wrote a separate deep-dive on that: How to Stop Calcium From Hardening Your Arteries — Without Drugs.
Disclaimer: This is my personal experience and documentation for educational purposes only. I am not a doctor or medical professional. hs-CRP results vary and should be interpreted in the context of your full health history. If you have cardiovascular disease, are taking medications, or are considering changes to your treatment plan, consult a qualified healthcare provider. The supplement information in this post is general education — talk to your doctor before starting any new supplementation, especially if you have existing health conditions. Do your own research and listen to your body.
Related Posts:
- How to Stop Calcium From Hardening Your Arteries — Without Drugs — The natural protocol for stopping arterial calcification: K2, magnesium, vitamin D, and why the order matters
- When Your Body Stops Playing by the Old Rules — How hypoxic breathwork + walking creates a cardiovascular training effect without running
- The Belly Fat That Wouldn't Leave — Why visceral fat is a nervous system problem, not a diet problem
- Zero Awakenings at 44 — How my sleep self-corrected after nervous system training
References
Huang, Y., Liu, H., Sun, L., et al. (2018). High-sensitivity C-reactive protein in aging Chinese adults: distribution and correlates from a longevity area. Immunity & Ageing, 15(1), 18. https://link.springer.com/article/10.1186/s12979-018-0126-7
Irwin, M.R., Wang, M., Campomayor, C.O., et al. (2006). Sleep deprivation and activation of morning levels of cellular and genomic markers of inflammation. Archives of Internal Medicine, 166(16), 1756-1762. https://pubmed.ncbi.nlm.nih.gov/17187297/
Ridker, P.M., Buring, J.E., Rifai, N., & Cook, N.R. (2002). Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: The Reynolds Risk Score. New England Journal of Medicine, 347(20), 1557-1565. https://pubmed.ncbi.nlm.nih.gov/12432042/
Ridker, P.M., Danielson, E., Fonseca, F.A.H., et al. (2008). Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein (JUPITER trial). New England Journal of Medicine, 359(21), 2195-2207. https://www.nejm.org/doi/full/10.1056/NEJMoa0807646
Ridker, P.M., Bhatt, D.L., Pradhan, A.D., et al. (2023). Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy. Circulation, 147(14), 1108-1117. https://www.ahajournals.org/doi/10.1161/CIRCULATIONAHA.123.066213
Ridker, P.M., Bhatt, D.L., Pradhan, A.D., et al. (2024). Inflammation, cholesterol, lipoprotein(a), and 30-year cardiovascular outcomes in women. New England Journal of Medicine, 391(22), 2087-2098. https://www.nejm.org/doi/full/10.1056/NEJMoa2405182
Rifai, N., Buring, J.E., Lee, I.M., et al. (2005). Is C-reactive protein specific for vascular disease in women? New England Journal of Medicine, 352(15), 1601-1603. https://www.nejm.org/doi/full/10.1056/NEJM200504143521525